How controlled is your asthma, really?
Five questions. Your clinical picture, instantly.
Answer five validated questions about your symptoms. A radial control gauge updates in real time, ending with a personalized clinical interpretation — before you share a single contact detail.
Well Controlled
Your asthma appears well managed. Annual spirometry and a trigger review will keep it that way.
How often do nighttime symptoms wake you?
How many times per week do you use a rescue inhaler?
Does asthma limit your physical activity?
How would you rate your overall asthma control?
When did you last have a spirometry (lung function) test?
Your answers are private. No account required to see your score.
When your immune system mistakes the air for an enemy
IgE-mediated triggers — dust mites, mold, pet dander, pollen — drive 60% of adult asthma. Identifying the exact sensitization profile changes everything.

Dr. Priya Nair
MD, FCCP — Board-Certified Pulmonologist
Allergic & Immunologic Asthma
“Most patients I see have been on the same step-2 regimen for years without a single skin prick or specific IgE panel. Once we map the allergen landscape, we can switch from daily suppression to targeted desensitization — and many patients halve their controller dose within six months.”
| Allergic Asthma | Outdated Assumption | Current Evidence |
|---|---|---|
| Diagnosis approach | Spirometry alone, symptom diary | Full allergen panel (ImmunoCAP) + fractional exhaled NO (FeNO) measurement |
| First-line treatment | SABA + low-dose ICS indefinitely | Allergen immunotherapy (sublingual or SCIT) alongside step-appropriate ICS |
| Trigger avoidance | Generic 'avoid dust and pets' advice | Personalized avoidance protocol based on sensitization profile and home assessment |
| Biologic eligibility | Biologics reserved for hospitalized patients only | Anti-IgE (omalizumab) indicated when ≥1 exacerbation/year with confirmed allergic phenotype |
| Follow-up interval | Annual check-up if 'stable' | Quarterly FeNO + peak flow trending, adjusted by allergen season |
The athlete who quietly stopped competing
EIB affects 1 in 10 adults and up to 40% of elite athletes. Most never receive a formal EVH challenge — they just accept the ceiling.

Dr. Marcus Webb
MD, PhD — Pulmonary & Sports Medicine
Exercise-Induced Bronchoconstriction
“The rescue inhaler before a race is not a treatment plan. Eucapnic voluntary hyperpnea testing gives us an objective bronchoprovocation threshold, and from there we can build a pre-exercise protocol, a controller regimen, and a return-to-sport timeline — not a permission slip to keep suffering.”
| Exercise-Induced Bronchoconstriction | Outdated Assumption | Current Evidence |
|---|---|---|
| Diagnosis standard | Self-reported symptoms + empiric albuterol | Eucapnic voluntary hyperpnea (EVH) or exercise challenge with spirometry pre/post |
| Pre-exercise protocol | 2 puffs albuterol 15 min before activity — every time | Individualized warm-up protocol + SABA only as needed; ICS/LABA if daily use |
| Cold/dry air management | Avoid outdoor exercise in winter | Humidified balaclava + airway conditioning; activity restriction rarely needed |
| Return to sport | Indefinite restriction or trial-and-error | Objective EVH threshold guides sport-specific training load and medication titration |
| Anti-doping compliance | Undisclosed SABA use in competitive athletes | TUE documentation + WADA-compliant controller selection from the outset |
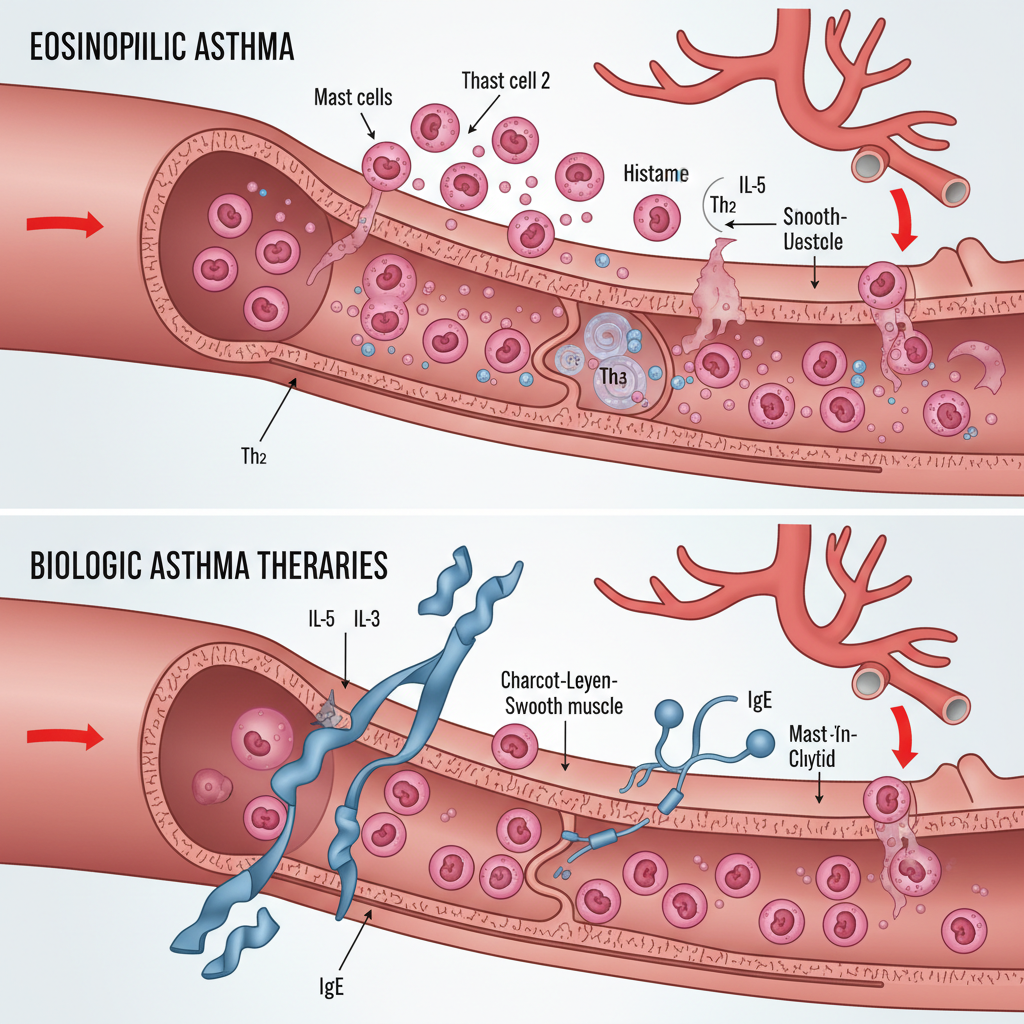
When standard controllers stop working
Eosinophil-driven inflammation underlies ~50% of severe asthma. Blood eosinophil count ≥300/μL is the gateway to a biologic that can eliminate exacerbations entirely.
Dr. Amara Osei
MD, DAABIM — Severe Asthma & Biologics
Eosinophilic & Biologic Asthma
“A patient on 2,000 mcg/day of ICS with three ER visits last year is not a compliance problem. They are a phenotyping problem. A single blood eosinophil count and FeNO can identify who will have a 70% exacerbation reduction on mepolizumab — and that information should take days to obtain, not years.”
| Severe Eosinophilic Asthma | Outdated Assumption | Current Evidence |
|---|---|---|
| Phenotyping workup | Escalate ICS dose, add LABA, observe | Blood eos + FeNO + sputum cytology + SNOT-22 (comorbid CRS) at step 4/5 |
| Biologic selection | Biologics as last resort after OCS dependency | Anti-IL-5 (mepolizumab/benralizumab) or anti-IL-4Rα (dupilumab) at step 5, guided by biomarkers |
| Oral corticosteroid use | Maintenance OCS accepted as 'controlled' | OCS-sparing is a primary biologic endpoint; ≥50% dose reduction expected within 6 months |
| Comorbidity management | Treat asthma; refer CRS separately | Unified airway approach — dupilumab addresses both CRS with polyps and Type-2 asthma simultaneously |
| Response monitoring | Symptom diary and patient-reported control | Serial blood eos + FeNO + ACQ-6 every 3 months to titrate or switch biologic |
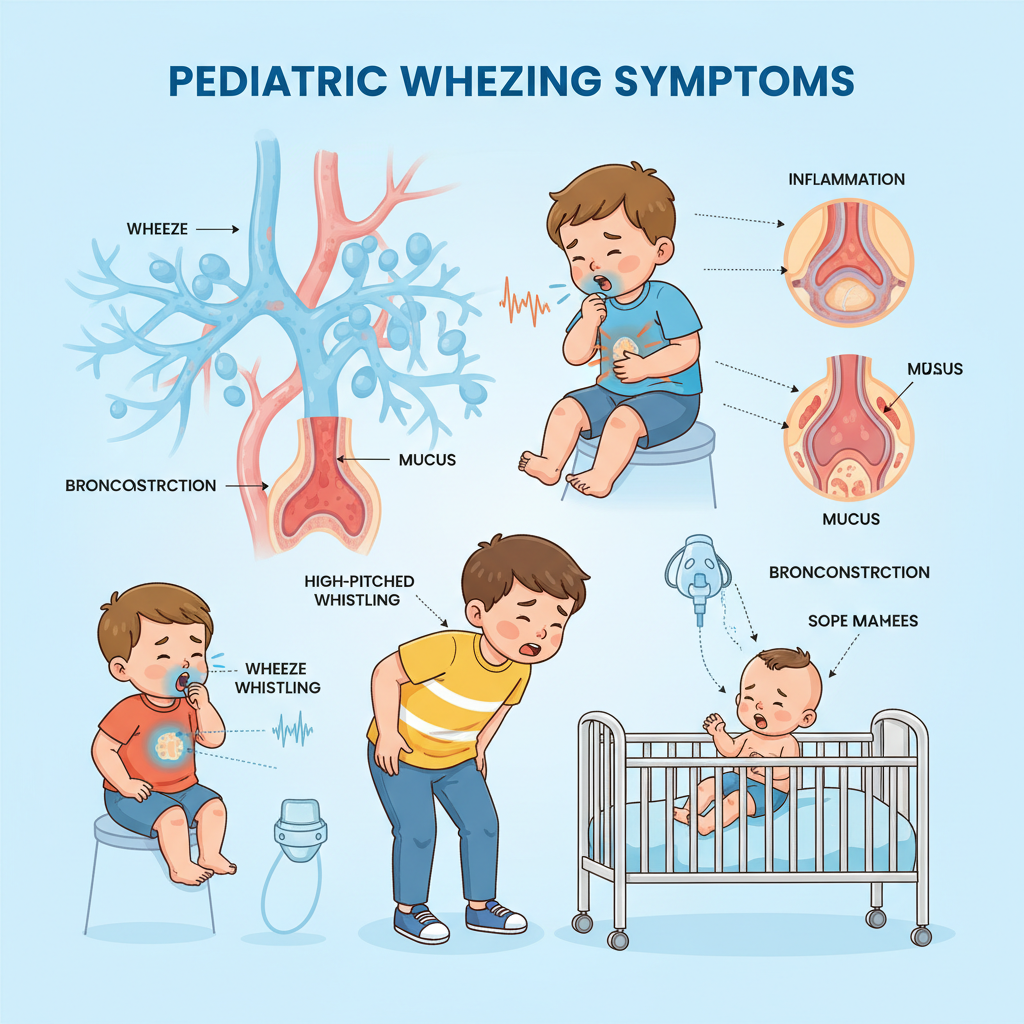
The 2am call that shouldn't keep happening
Recurrent wheeze before age 5 is not 'something they'll outgrow.' Early phenotyping determines which children benefit from controller therapy — and which don't need it.
Dr. Sofia Reyes
MD, FAAP — Pediatric Pulmonology
Pediatric & Preschool Wheeze
“Parents come to me exhausted. They've been to the ER twice, they have a nebulizer on the nightstand, and their pediatrician says 'wait and see.' A Childhood Asthma Predictive Index score and an impulse oscillometry session — which takes 45 seconds and requires no forced effort — tells me whether this child needs a daily controller or just an action plan for viral episodes. That's not waiting. That's knowing.”
| Pediatric Wheeze | Outdated Assumption | Current Evidence |
|---|---|---|
| Diagnosis in under-5s | Cannot diagnose asthma before age 5; observe only | Childhood API + impulse oscillometry (IOS) enables phenotyping and risk stratification at age 2+ |
| Controller threshold | ICS for any child with ≥2 wheeze episodes | Intermittent ICS (PREEMPT protocol) for viral-triggered wheeze; daily ICS only for multi-trigger or atopic phenotype |
| Nebulizer vs. MDI | Nebulizer preferred for young children | MDI + valved holding chamber (VHC) is equally effective and reduces treatment time from 20 min to 2 min |
| School/daycare management | Written action plan with fixed dose instructions | Color-coded individualized asthma action plan with weight-based dosing and trigger-specific instructions |
| Long-term prognosis | Most children outgrow asthma by adolescence | 50% of childhood wheezers persist into adulthood; early controller therapy reduces airway remodeling risk |
Breathe Clinic — Austin, TX
The tightness releasing. The air arriving.
The world suddenly wider.
Board-certified pulmonologists who map every trigger, measure every airflow curve, and build treatment plans around your life — not a standard protocol.
4,200+
Patients treated
94%
Exacerbation reduction
< 5 days
Avg. time to appointment